
A new Nature Biotechnology paper describes the process of engineering a lab-grown esophagus that can safely replace a full section of the native organ and restore normal functions, including swallowing, in a growing animal without requiring immunosuppression. The paper, which is titled “Functional integration of an autologous engineered esophagus in a large-animal model,” describes “an integrated strategy to engineer a 2.5-cm esophageal segment by microinjecting autologous pericyte-like myogenic precursors and fibroblasts in a decellularized porcine scaffold to repair circumferential defects in 10-kg minipigs … modeling pediatric use.”
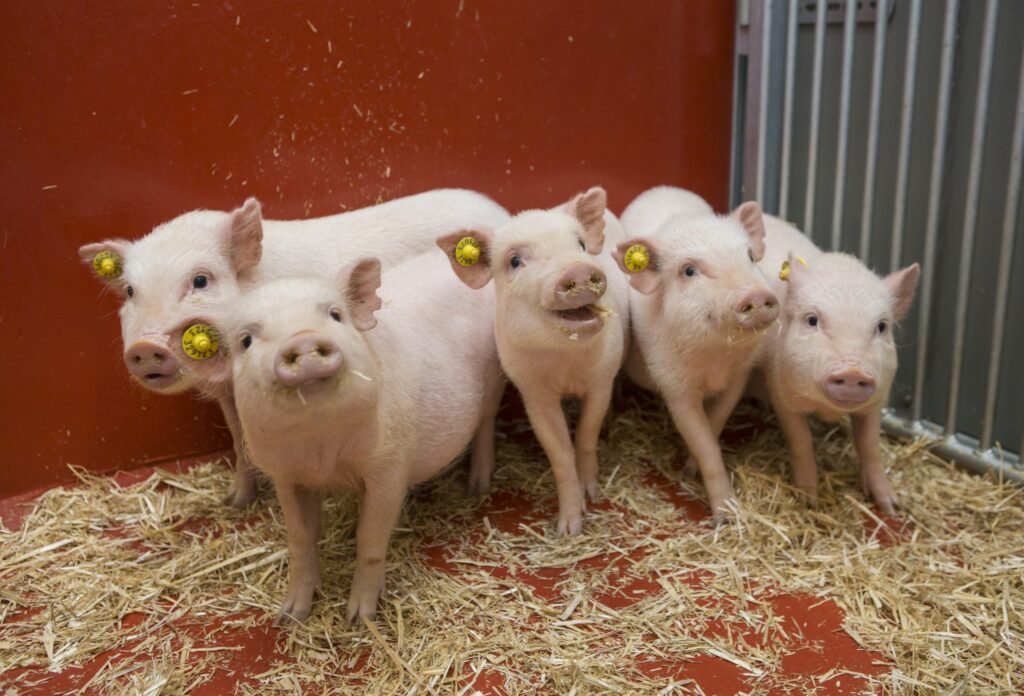
According to scientists from Great Ormond Street Hospital (GOSH) and University College London (UCL) who led the study, their work demonstrates for the first time that a donor pig esophagus can be decellularized, repopulated with the recipient pig’s own cells and implanted in a growing, large-animal model. Other studies have previously shown parts of this technology but this marks the first time that the full process has been completed with this level of success, they said.
Importantly, this development is a major leap towards creating personalized regenerative treatments for children born with life threatening esophageal conditions. Specifically, it could benefit children born with a condition called long-gap esophageal atresia (LGOA). People with this condition have an interrupted esophagus with a wide gap between the upper and lower segments. Patients cannot survive without surgery, but the gap is often too large to close immediately after birth. As a work around, babies with LGOA typically have a feeding tube placed directly into their stomach, so that they can receive adequate nutrition while their hospital teams develop a treatment plan.
Surgery is an effective treatment approach but is not without challenges. Current surgical options are complex and invasive processes that involve repositioning the stomach or intestine to bridge the gap. While many children achieve good outcomes, both options have significant short- and long-term complications including breathing and gastrointestinal problems. As such, better options with reduced risk of complications to patients are still needed.
Engineered tissue from donor pigs could be one of those options. In this process, the donor pig esophagus, which acts as base for the new organ, is stripped of all its cells while keeping the underlying support structure intact. Next this scaffold is repopulated with a recipient pig’s muscle cells. The cells, which are taken from a small biopsy, are multiplied in the lab and injected directly into the scaffold. The graft is then placed in a bioreactor for a week. During this time the cells settle, spread, and adapt to their new environment. In all, the process takes two months to complete.
According to results reported in the paper, all eight recipient pigs in the study survived the critical first 30 days following transplant. By the six-month mark, the lab-grown grafts had developed functional muscle, nerves, and blood vessels that allowed the transplanted esophagus to contract and move food like a native organ so that the recipient animals could eat normally. The scientists note that some animals experienced narrowing of the organ but these were successfully managed through endoscopy. Additionally, the team used spatial transcriptomics to map the genes present in the implanted tissue. They showed that the genes turned on in the transplanted esophagus were similar to what would be expected in a native organ.
If this technology can be safely adapted for use in humans, different sizes of donor pig scaffolds could be stored ready to be developed and personalized for use as needed. Biopsy cells could be taken from the child when the feeding tube is placed and incorporated into the scaffold in exactly the same way as described in the paper.
“Our technology could allow us to build a child a new esophagus, using their own cells, collected in a surgery they are having anyway, combined with a ready-prepared scaffold from pig tissue,” said Marco Pellegrini, PhD, senior researcher at UCL GOS Institute of Child Health and a co-lead on the study. “Because the graft contains the child’s own muscle progenitor cells, it would be recognized as their own tissue. This means it could grow with them over time, without the risk of rejection and without the need for long-term immunosuppression.”
The team is now refining the process to generate longer grafts, standardizing manufacturing, reducing manual steps, and carrying out further safety testing. Further studies will focus on tracking the cells on the tissue, optimizing blood flow and preparing the therapy for first-in-human trials. They hope to begin a research trial for the technology in the next five years.