
Foundational preclinical data generated through research, hypothesis development, testing, and reiteration leads to the development of new approaches to treat the most recalcitrant solid tumors. As today’s next-generation therapies make their progression through clinical trials and market acceptance, another invaluable feedback loop of patient data ensues to impact even more generational advances.
Cancer—especially solid tumors—is a heterogeneous disease with many obstacles that thwart treatment, including the tumor microenvironment and its immunosuppressive effects. No one therapy is ideal for every cancer patient or indication, despite stratification attempts. And, although meaningful, personalized approaches are simply not economically feasible as a broad approach.
So, scientists do what they do best. They innovate and build on accumulated knowledge, including leveraging existing technologies in new combinations, to develop new ideas that address unmet needs. New approaches look at cellular biology and immunology for their inspiration and build on the power of existing technology and therapies. These generational advances are another step toward not only remission but also potential cures.
Engineering γδ T cells
Many existing cellular immunotherapies cannot persist in the presence of standard-of-care (SOC) treatments such as chemotherapy and radiation. In aggressive cancers like glioblastoma, and in the upfront setting when the immune system is at its strongest, these SOC treatments create an immune-hostile environment that rapidly depletes conventional immune cells, limiting the effectiveness of most immunotherapy approaches.
The DeltEx Drug Resistant Immunotherapy (DeltEx DRI) platform was developed to advance gd T cell therapies into indications with high unmet need, in particular, highly heterogeneous solid tumors that are protected by physical barriers and have a highly immunosuppressive tumor microenvironment.
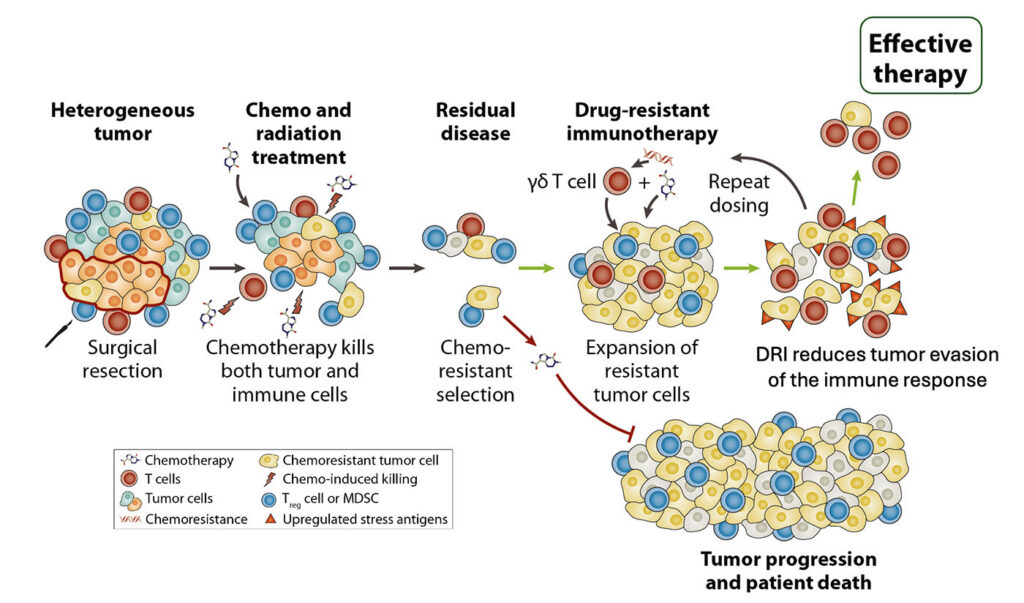
“The most powerful cancer treatment is to attack a tumor upfront with everything in our arsenal, when the tumor is at its most vulnerable and not heavily pretreated,” said William Ho, CEO and co-founder at IN8bio. “Immunotherapy does not need to displace existing SOC to succeed. Clinical workflows, treatment sequencing, or physician practice patterns can stay in place. Our simple concept is an elegant approach to overcoming the challenges of solid tumor cancers.”
IN8bio engineers gd T cells to be chemotherapy resistant, enabling them to survive, expand, and remain functional even when administered concurrently with standard treatments. This allows for repeat dosing and sustained immune pressure, rather than a single transient exposure.
IN8bio’s pipeline includes multiple clinical and preclinical programs spanning both oncology and autoimmune diseases.
In their lead INB-200/400 program in glioblastomas, the gd T cells are engineered to be resistant to Temozolomide (TMZ), the SOC chemotherapy used in newly diagnosed glioblastoma. Updated Phase I and Phase II data, observed across multiple clinical centers, show that repeat dosing of DeltEx DRI gd T cells can be delivered without significant adverse events, including dose-limiting toxicities, cytokine release syndrome, and immune effector cell-associated neurotoxicity.
Patients treated with repeat doses of DeltEx DRI gdT cells demonstrated a 97% improvement in median progression-free survival compared to the SOC control cohort, a major improvement since the last glioblastoma drug approval of TMZ in 2005.
The company employs a controlled, closed-system manufacturing workflow that supports expansion, activation, genetic engineering, and cryopreservation of gd T cells, while maintaining strict quality controls across batches. The modular platform is scalable and adaptable across multiple indications, as well as autologous and allogeneic products.
Installing a beacon
Designed to solve two of the hardest problems in solid tumors, the Flare platform is a dual-component system that finds a clean tumor-specific target and overcomes an immunosuppressive tumor microenvironment. An IV-administered, tumor-specific virus selectively infects tumor cells and installs a protein tag, called a Flare, on their surface. That Flare acts as a beacon that can be recognized by a targeting therapy that eliminates the virally infected cells.
According to Barbra Sasu, PhD, CSO at Dispatch Bio, in their first program, DISP-10, the Flare is a modified version of BCMA. The targeting component is a clinically validated BCMA CAR T cell, originally developed for myeloma. Not only does the virus install the target, it also creates local inflammation that supports CAR T activation, expresses immune-stimulating payloads to enhance both CAR T and endogenous immune activity, and helps recruit immune cells into the tumor microenvironment.
Once CAR T cells lyse infected tumor cells, thousands of new viral particles are released locally, infecting surrounding tumor cells and tagging them with Flare. “This positive feedback loop—new Flare expression, renewed immune activation, and continued CAR T-mediated elimination of tumor cells—allows the platform to essentially work to target the tumor from the inside out,” Sasu pointed out.
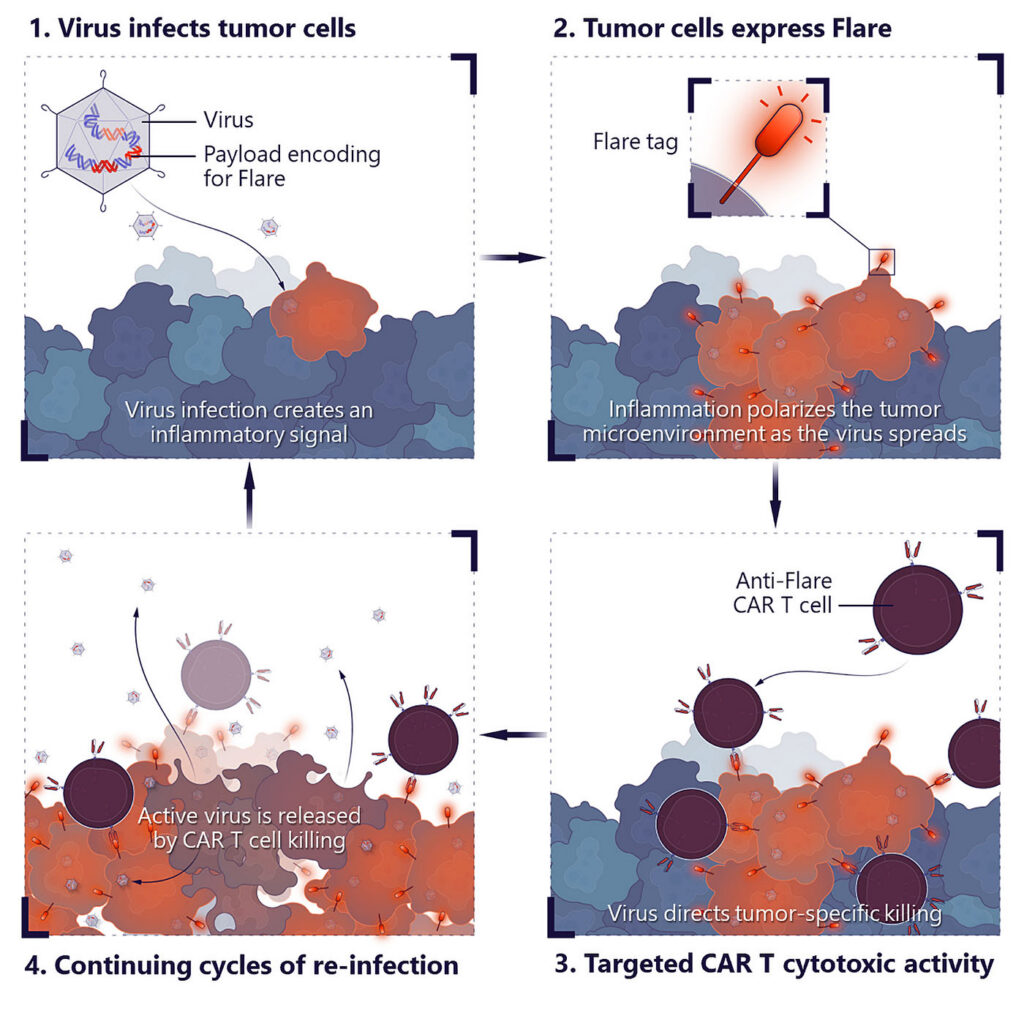
An inflammatory environment within the tumor and immune-stimulating payloads help CAR T cells remain active, proliferate, and resist exhaustion. Together, these effects support both improved efficacy and persistence in settings where CAR T cells have historically struggled.
The tumor-specific virus has tropism for about 90% of solid tumors, those of epithelial origin. “Because the virus can selectively infect these tumors and install the same Flare target, we are able to apply a single targeting strategy across many different indications, essentially turning many solid tumors into one therapeutic opportunity,” highlighted Sasu.
Preclinical studies demonstrated synergy between the viral component and CAR T cells. Enhanced viral amplification, increased Flare expression, and robust tumor cell clearance in vitro were observed. In vivo, the cytokine and chemokine payloads of the virus support immune activation and can increase T cell cytotoxicity and help prevent exhaustion.
DISP-10 has an open IND in the U.S., and the company, working with Bristol Myers Squibb using ide-cel, expects to begin a Phase I study in solid tumor patients in 2026, and with CARsgen on a related program in China using zevor-cel.
Utilizing host defense peptides
“We asked how we could create a strong local and systemic immune response by selectively destroying tumor cells,” said Baldur Sveinbjørnsson, PhD, CSO, Lytix Biopharma. This led to the discovery and improvement of the synthetic oncolytic peptide Ruxotemitide (LTX-315/VP-315), a 9-mer peptide derived from a group of molecules, found in all living species, that plays a key role in the innate immune system as host-defense peptides.
Ruxotemitide primarily acts by selectively disrupting cancer cell membranes through interactions between the peptide’s cationic amino acid side chains and the negatively charged membrane components that are more abundant in cancer cells.
Mechanistically, first the peptides induce rapid immunogenic cell death, releasing tumor antigens and danger-associated molecular patterns (DAMPs: endogenous molecules released by damaged or dying cells that trigger innate immune responses) into the tumor microenvironment. Second, this local tumor destruction activates an innate immune response, followed by the recruitment and priming of adaptive immune cells. This process turns an immunologically “cold” tumor into a “hot,” inflamed one.
Importantly, an abscopal effect, characterized by the shrinkage or elimination of untreated distant lesions, has been observed in both experimental metastasis models and clinical trials.
Oncolytic peptides are chemically synthesized, non-replicating molecules with predictable pharmacology and no risk of uncontrolled amplification. Their activity is not affected by host neutralizing antibodies, and their mechanism of action does not depend on specific receptors or tumor-specific mutations.
“These features enable more consistent intratumoral immune activation and make the platform well-suited for repeated dosing and combination regimens,” said Sveinbjørnsson.
The target-agnostic platform is broadly applicable to solid tumors accessible via intratumoral injection. Clinically, Ruxotemitide has been tested in various solid tumors as monotherapy and in combination with immune checkpoint inhibitors, resulting in durable responses, including solid tumors refractory to immune checkpoint inhibitors.
In addition, results from a Phase II trial for Basal Cell Carcinoma demonstrated strong efficacy, including a 97% response rate and over 50% complete histological clearance, with a favorable safety profile.
“Encouraged by our initial clinical findings combining intratumoral Ruxotemitide and pembrolizumab (Keytruda) in patients with advanced or metastatic melanoma, our strategic focus has shifted,” elaborated Sveinbjørnsson. The NeoLipa study (NCT06651151) is an academic investigator-initiated Phase II clinical trial investigating the combination therapy as a neoadjuvant treatment for resectable stage III-IV melanoma. Interim data are promising.
Discovering new targets
Despite the emphasis on personalized treatments based on specific driver mutations, significant overlap exists in how cancers function. “Cancer may start from different mutations, but it must accomplish the same biological objectives. That convergence creates shared vulnerabilities,” said Jon Moore, PhD, CSO at Epitopea.
These changes frequently involve epigenetic regulation, alternative splicing, and broader shifts in the proteome. As a result, conservation of certain aberrantly expressed tumor-specific antigens (aeTSAs) occurs across patients with the same tumor type—even if those proteins themselves are not classical drivers.
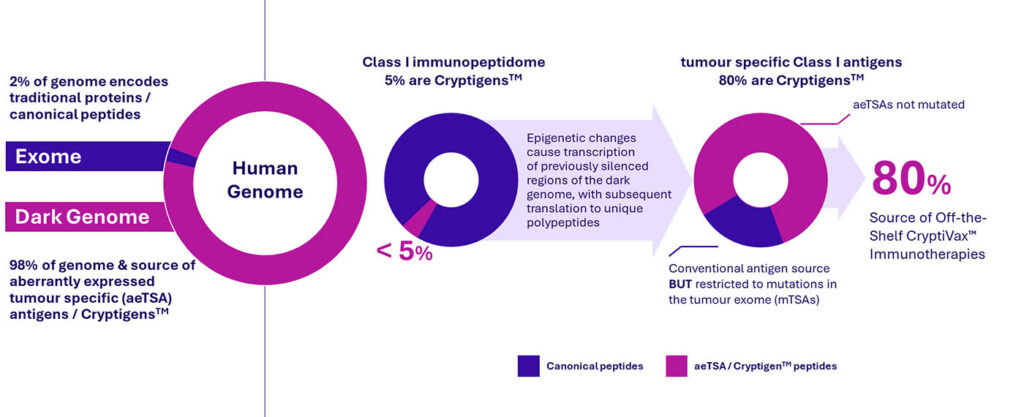
“We believe these proteins represent therapeutic targets. Precision therapeutics has traditionally explored only two percent of the genome. The remaining transcribed genome represents a vast, untapped opportunity,” said Alan Rigby, PhD, CEO at Epitopea. “Advances in deep, empirical mass spectrometry now permit a deeper interrogation of the MHC presented repertoire critical for immune recognition.”
Importantly, transcripts expressed in thymic medullary epithelial cells, which train the immune system to tolerate self, and/or determined to be expressed in the Adult Genotype-Tissue Expression (GTEx) dataset, are subtracted. aeTSAs derived from this expanded genomic space are highly cancer-specific, shared across patient subsets diagnosed with the same tumor type, and more abundant and immunogenic than previously discovered conventional neoantigens.
Epitopea’s vaccine platform incorporates iterative optimization principles borrowed from traditional hit-to-lead, lead optimization, and development candidate validation metrics leveraged in many small-molecule discovery campaigns. “We optimize not just the antigenic peptide but also other aspects of the construct that influence how these aeTSAs are presented to the immune system,” explained Rigby. This enhances T cell receptor diversity and promotes memory T-cell formation, critical for durability of response, which, ultimately, translates into meaningful clinical responses.
Epitopea’s first clinical program will be a Phase I, first-in-human trial in homologous recombination-proficient (HRP) high-grade serous ovarian cancer, beginning in 2026 in the U.K. HRP patients represent about 50% of ovarian cancer cases that do not benefit from PARP inhibitors. “In HRP ovarian cancer, patients currently have few precision-based options. We aim to change that in a first-line maintenance setting,” said Rigby.
The off-the-shelf RNA-based immunotherapies are built by adapting and optimizing the beads-on-a-string approach similar to those deployed in personalized cancer vaccines. The number of aeTSAs and the degree of sharing within a tumor indication suggest that, for many indications, a cancer therapy comprised of 25 aeTSAs would support a predicted tumor-specific median patient presentation.
Harnessing cytotoxic proteins
At the core of the targeted Granzyme B immunotherapy (TGI) platform is the replacement of synthetic exogenous toxins with the immune system’s own primary effector of cell death. The TGI platform harnesses the immune system’s primary potent cytotoxic protein, Granzyme B (GrB), as a safe and effective payload for targeting cancer and other cell proliferative diseases.

By fusing natural GrB to a human IgG1 heavy chain fragment that is, in turn, fused to any antigen-targeting scFv or ligand, the platform delivers a fusion protein with universal use without immune cells facilitating targeted delivery. The payload is quickly endocytosed following binding to the target, induces apoptosis by three independent, irreversible pathways, and stimulates immunogenic cell death resulting in bystander killing of neighboring tumor cells.
GrB cannot enter the cell non-specifically and is cytotoxic only once internalized directly into the cytosol, allowing for optimized dosing and sustained tumor suppression without the safety trade-offs associated with non-specific payload release.
Unlike ADCs, GrB is enzymatically active without release from the cell-targeting carrier, has a very high therapeutic index, and is not affected by pre-existing chemo-resistance mechanisms. Animal studies have demonstrated long-term tumor suppression at doses of 20-40 mg/kg and a maximum tolerated dose >500 mg/kg, thus providing a wide therapeutic window for dose escalation.
Plus, manufacturing of GrB fusion proteins uses a streamlined, recombinant mAb process allowing production with the consistency, robustness, and scalability of established biologics.
“Our strategy departs from conventional ADC design by maintaining GrB as a constant immune effector. Swapping antigen-specific targeting antibodies or ligands separates delivery from mechanism, to enable a true platform universal approach,” said Claire Thuning-Roberson, PhD, CEO, AbBC Therapies. “GrB-based therapeutics represent a generational advance.”
The cytotoxic effect of GrB on cells or in tumor xenograft models is consistent and reproducible regardless of target or tumor type. “This is not surprising. The technology simply delivers GrB to the cell where it is quickly internalized and produces immediate cytotoxicity,” Thuning-Roberson emphasized.
Dramatic tumor regression was seen in mouse xenograft models when targeting Fn14, CEA, and mesothelin. Taxol, cisplatin, and MDR-resistant cell lines remained sensitive to GrB.
Scientists remain determined to turn cancer, even the most difficult to treat cases, into a curable disease as the technologies highlighted in this article demonstrate. These innovative approaches, and others in development, have the potential to positively impact millions of lives. Only time and continued clinical trials will reveal the outcomes.

